
Main highlights:
The length of diagnosis, and not age, is the main predictor for PLWH to suffer from multiple comorbidities1
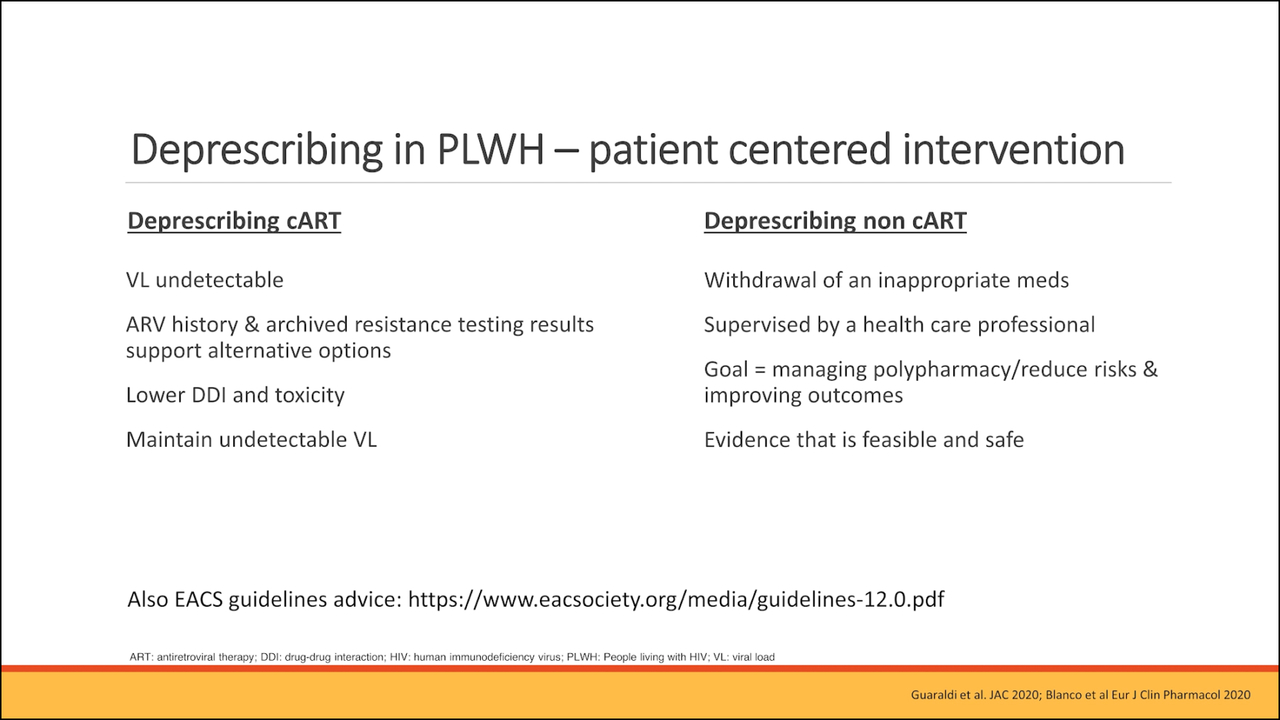
De-prescription of cART and non cARTs is increasingly more important, coupled to exploring newer drugs like dolutegravir and doravirine that are characterized by less drug-drug interactions2-4
The MDT of Chelsea and Westminster Hospital links to wider care teams and specialties, including the GP.5
The MDT of Chelsea and Westminster Hospital conducts fragility and geriatric assessment and follows a 7-point clinical pathway for PLWH over 50 y.o, providing them with personalized care5
(re)watch the summary of Dr Boffito’s conference

Dive into the different themes addressed by Dr Boffito
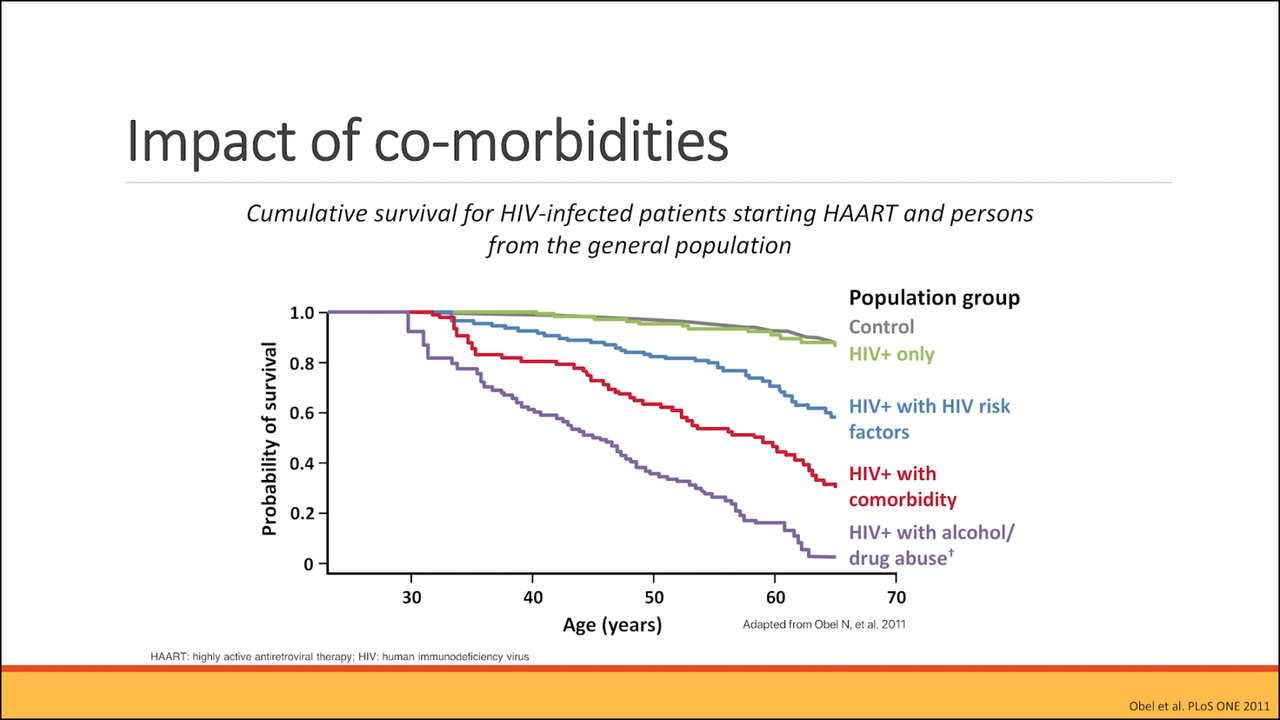
Aging HIV population and the impact of their comorbidities
What are the impact of co-morbidities on aging HIV patients?3
Clinical pathway in people living with HIV; part 1
Dr. Boffito and her team implemented a clinical pathway checklist of 7 items to conduct on PLWH over 50’s5
Part 1 covers: drug history and interactions, renal function, endocrine function and cancer screening
Clinical pathway in people living with HIV; part 2
Dr. Boffito and her team implemented a clinical pathway checklist of 7 items to conduct on PLWH over 50’s5
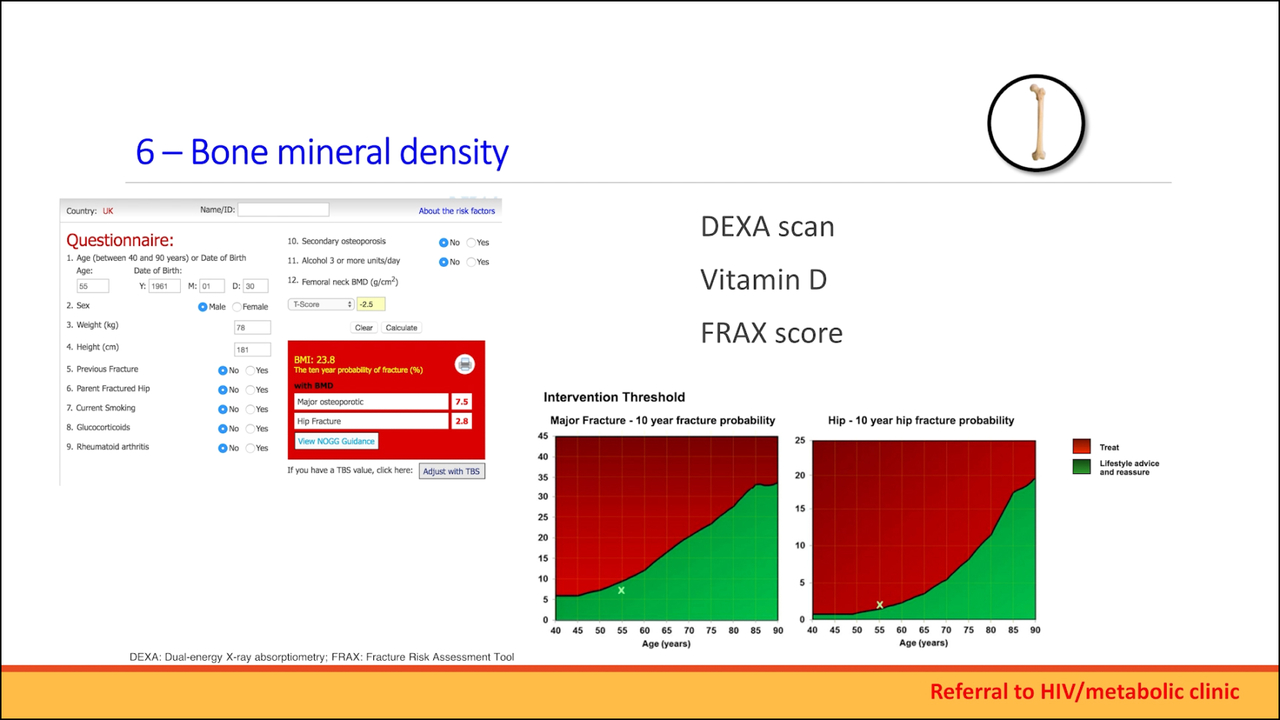
Part 2 covers: cardiovascular risk assessment, bone mineral density and cognitive function
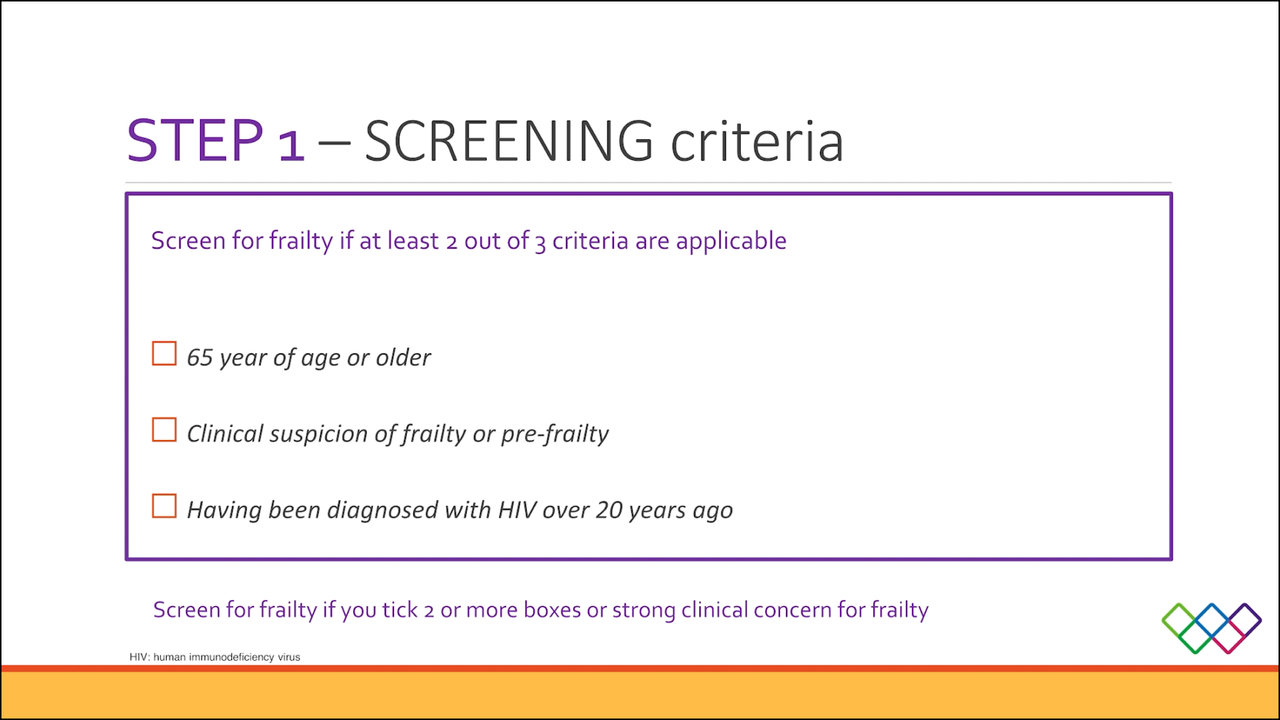
Frailty pathway for people living with HIV
A multidisciplinary team (MDT) consultation using the principles of comprehensive geriatric assessment has been setup in a geriatric/HIV clinic at the Chelsea and Westminster hospital, where frailty is assessed using Rockwood Clinical Frailty Scale5

Meet the expert
Prof Marta Boffito MD, PhD, FRCP, MBA
Consultant Physician; Clinical Director HIV, Sexual and Gender Health, Dermatology
Chelsea and Westminster Hospital
Originally interested in psychiatry, Boffito became interested in infectious diseases while in medical school in Italy.
“I became passionate about HIV because although at that time there was no effective antiretroviral treatment, the empathy around the disease and the motivation to find treatment were astonishing”, states Boffito. Her passion for HIV was further strengthened when she pursued infectious diseases training in Italy and at the San Francisco General Hospital, CA, USA. Driven by a desire to improve ARV treatment, Boffito decided to pursue a PhD in clinical pharmacology at the University of Liverpool, Liverpool, UK. After completing her PhD, Boffito began working as a research fellow at the Chelsea and Westminster Hospital, London, UK, where she is currently the clinical director of HIV, sexual and gender health, and dermatology services.6
Written summary




Download our written summary
that also includes the Frailty pathway and frailty scale used by Dr Boffito and her multidisciplinary team
ART: antiretroviral therapy; ARV: antiretroviral; cART: combination ART; FRCP: fellow of the royal college of physicians; GP: general practitioner; HIV: human immunodeficiency virus; MBA: master in business administration; MD: medical doctor; MDT: multidisciplinary team; PhD: Doctor of Philosophy; PLWH: people living with HIV.
- Dr Marta Boffito, expert opinion shared during the presentation held in the CHU of Liege
- Smit M, et al. Future challenges for clinical care of an ageing population infected with HIV: a modelling study. Lancet Infect Dis. 2015 Jul;15(7):810-8
- Schouten J, et al. Cross-sectional comparison of the prevalence of age-associated comorbidities and their risk factors between HIV-infected and uninfected individuals: the AGEhIV cohort study. Clin Infect Dis. 2014 Dec 15;59(12):1787-97
- Deeks SG, et al. HIV infection, antiretroviral treatment, ageing, and non-AIDS related morbidity. BMJ. 2009 Jan 26;338:a3172
- Guaraldi et al. Presentation done at the 18th IWCADRH 2016 . Available on: https://www.natap.org/2016/AdverseReactComor/AdverseReactComor_15.htm. Last accessed June 2024
- Kazi F, et al. Marta Boffito-The happy warrior. Lancet Infect Dis. 2023 Aug;23(8):896.
Please consult the full prescribing information before prescribing or delivering the product.
1. NAME OF THE MEDICINAL PRODUCT Delstrigo 100 mg/300 mg/245 mg film-coated tablets. 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Each film-coated tablet contains 100 mg of doravirine, 300 mg of lamivudine (3TC), and 245 mg of tenofir disoproxil as tenofovir disoproxil fumarate (TDF). Excipient with known effect: Each film-coated tablet contains 8.6 mg lactose (as monohydrate). For the full list of excipients, see section 6.1. 3. PHARMACEUTICAL FORM Film-coated tablet (tablet). Yellow, oval-shaped, tablet of dimensions 21.59 mm x 11.30 mm, debossed with the corporate logo and 776 on one side and plain on the other side. 4. CLINICAL PARTICULARS 4.1 Therapeutic indications Delstrigo is indicated for the treatment of adults infected with human immunodeficiency virus type 1 (HIV‑1) without past or present evidence of resistance to the non-nucleoside reverse transcriptase inhibitors (NNRTI) class, lamivudine, or tenofovir (see sections 4.4 and 5.1). Delstrigo is also indicated for the treatment of adolescents aged 12 years and older weighing at least 35 kg who are infected with HIV-1 without past or present evidence of resistance to the NNRTI class, lamivudine, or tenofovir and who have experienced toxicities which preclude the use of other regimens that do not contain tenofovir disoproxil (see sections 4.4 and 5.1). 4.2 Posology and method of administration Therapy should be initiated by a physician experienced in the management of HIV infection. Posology The recommended dose of Delstrigo is one 100/300/245 mg tablet taken orally once daily with or without food. Dose adjustment If Delstrigo is co-administered with rifabutin, the doravirine dose should be increased to 100 mg twice daily. This is achieved by adding one 100 mg tablet of doravirine (as a single agent), to be taken approximately 12 hours apart from the dose of Delstrigo (see section 4.5). Co-administration of doravirine with other moderate CYP3A inducers has not been evaluated, but decreased doravirine concentrations are expected. If co-administration with other moderate CYP3A inducers (e.g., dabrafenib, lesinurad, bosentan, thioridazine, nafcillin, modafinil, telotristat ethyl) cannot be avoided, one 100 mg tablet of doravirine should be taken daily, approximately 12 hours after the dose of Delstrigo (see section 4.5). Missed dose If the patient misses a dose of Delstrigo within 12 hours of the time it is usually taken, the patient should take Delstrigo as soon as possible and resume the normal dosing schedule. If a patient misses a dose of Delstrigo by more than 12 hours, the patient should not take the missed dose and instead take the next dose at the regularly scheduled time. The patient should not take 2 doses at one time. Special populations Elderly There are limited data available on the use of doravirine, lamivudine, and tenofovir disoproxil in patients aged 65 years and over. There is no evidence that elderly patients require a different dose than younger adult patients (see section 5.2). Special care is advised in this age group due to age associated changes such as decreases in renal function (see section 4.4). Renal impairment No dose adjustment of Delstrigo is required in patients with estimated creatinine clearance (CrCl) ≥ 50 mL/min. Delstrigo should not be initiated in patients with estimated CrCl < 50 mL/min (see sections 4.4 and 5.2). Delstrigo should be discontinued if estimated CrCl declines below 50 mL/min (see section 4.4). Patients with moderate or severe renal impairment require a dose interval adjustment of lamivudine and tenofovir disoproxil that cannot be achieved with the combination tablet (see sections 4.4 and 5.2). Hepatic impairment No dose adjustment of doravirine/lamivudine/tenofovir disoproxil is required in patients with mild (Child-Pugh Class A) or moderate (Child-Pugh Class B) hepatic impairment. Doravirine has not been studied in patients with severe hepatic impairment (Child-Pugh Class C). It is not known whether the exposure to doravirine will increase in patients with severe hepatic impairment. Therefore, caution is advised when doravirine/lamivudine/tenofovir disoproxil is administered to patients with severe hepatic impairment (see section 5.2). Paediatric population Safety and efficacy of Delstrigo in children aged less than 12 years or weighing less than 35 kg have not been established. No data are available. Method of administration Delstrigo must be taken orally, once daily with or without food and swallowed whole (see section 5.2). 4.3 Contraindications Hypersensitivity to the active substances or to any of the excipients listed in section 6.1. Co-administration with medicinal products that are strong cytochrome P450 CYP3A enzyme inducers is contraindicated as significant decreases in doravirine plasma concentrations are expected to occur, which may decrease the effectiveness of Delstrigo (see sections 4.4 and 4.5). These medicinal products include, but are not limited to the following: carbamazepine, oxcarbazepine, phenobarbital, phenytoin; rifampicin, rifapentine; St. John’s wort (Hypericum perforatum); mitotane; enzalutamide; lumacaftor. 4.8 Undesirable effects Summary of the safety profile In phase 3 clinical trials with doravirine plus 2 nucleoside reverse transcriptase inhibitors (NRTIs), the most frequently reported adverse reactions considered possibly or probably related to doravirine were nausea (4 %) and headache (3 %). Tabulated summary of adverse reactions The adverse reactions with doravirine plus 2 NRTIs from Phase 3 clinical trials (DRIVE-FORWARD, DRIVE-SHIFT and DRIVE-AHEAD) and postmarketing experience are listed below by body system organ class and frequency. Within each frequency grouping, undesirable effects are presented in order of decreasing seriousness. Frequencies are defined as very common (≥ 1/10), common (≥ 1/100 to < 1/10), uncommon (≥ 1/1 000 to < 1/100), rare (≥ 1/10 000 to < 1/1,000), very rare (< 1/10 000), or not known (cannot be estimated from the available data). Table 2: Tabulated summary of adverse reactions associated with doravirine/lamivudine/tenofovir disoproxil Frequency/ Adverse reactions: Infections and infestations: Rare: rash pustular. Blood and lymphatic systems disorders: Uncommon: neutropenia*, anaemia*, thrombocytopenia*; Very rare: pure red cell aplasia*. Metabolism and nutrition disorders: Uncommon: hypophosphataemia, hypokalaemia*; Rare: hypomagnesaemia, lactic acidosis*. Psychiatric disorders: Common: abnormal dreams, insomnia1; Uncommon: nightmare, depression2, anxiety3, irritability, confusional state, suicidal ideation; Rare: aggression, hallucination, adjustment disorder, mood altered, somnambulism. Nervous system disorders: Common: headache, dizziness, somnolence; Uncommon: disturbance in attention, memory impairment, paraesthesia, hypertonia, poor quality sleep; Very rare: peripheral neuropathy (or paraesthesia)*. Vascular disorders: Uncommon: hypertension. Respiratory, thoracic and mediastinal disorders: Common: cough*, nasal symptoms*; Rare: dyspnoea, tonsillar hypertrophy. Gastrointestinal disorders: Common: nausea, diarrhoea, abdominal pain4, vomiting, flatulence; Uncommon: constipation, abdominal discomfort5, abdominal distension, dyspepsia, faeces soft6, gastrointestinal motility disorder7, pancreatitis*; Rare: rectal tenesmus. Hepatobiliary disorders: Rare: hepatic steatosis*, hepatitis†. Skin and subcutaneous tissue disorders: Common: alopecia*, rash8; Uncommon: pruritus; Rare: dermatitis allergic, rosacea, angioedema*; Not known: toxic epidermal necrolysis. Musculoskeletal and connective tissue disorders: Common: muscle disorders*, bone mineral density decreased*; Uncommon: myalgia, arthralgia, rhabdomyolysis*‡, muscular weakness*‡; Rare: musculoskeletal pain, osteomalacia (manifested as bone pain and infrequently contributing to fractures)*, myopathy*. Renal and urinary disorders: Uncommon : increased creatinine*, proximal renal tubulopathy (including Fanconi syndrome)*; Rare: acute kidney injury, renal disorder, calculus urinary, nephrolithiasis, acute renal failure*, renal failure*, acute tubular necrosis*, nephritis (including acute interstitial)*, nephrogenic diabetes insipidus*. General disorders and administration site conditions: Common: fatigue, fever*; Uncommon: asthenia, malaise; Rare: chest pain, chills, pain, thirst. Investigations: Common: alanine aminotransferase increased9; Uncommon: aspartate aminotransferase increased, lipase increased, amylase increased, haemoglobin decreased; Rare: blood creatine phosphokinase increased. *This adverse reaction was not identified as an adverse reaction associated with doravirine from the Phase 3 clinical studies (DRIVE-FORWARD, DRIVE-AHEAD, DRIVE-SHIFT), but is included in this table as an adverse reaction based on the Summary of Product Characteristics of 3TC and/or TDF. The highest frequency category reported in the 3TC or TDF Summary of Product Characteristics (SmPC) of 3TC and/or TDF. The highest frequency category reported in the 3TC or TDF SmPC is used. †This adverse reaction was not identified as an adverse reaction associated with doravirine from the Phase 3 clinical studies (DRIVE-FORWARD, DRIVE-AHEAD, DRIVE-SHIFT), but was seen during post-marketing use of doravirine-containing regimens and is an adverse reaction listed in the SmPC of 3TC and TDF. The highest frequency category reported in the 3TC and TDF SmPCs is used. ‡This adverse reaction may occur as a consequence of proximal renal tubulopathy. It is not considered to be causally associated with tenofovir disoproxil in the absence of this condition. 1insomnia includes: insomnia, initial insomnia and sleep disorder. 2depression includes: depression, depressed mood, major depression, and persistent depressive disorder. 3anxiety includes: anxiety and generalised anxiety disorder. 4abdominal pain includes: abdominal pain, and abdominal pain upper. 5abdominal discomfort includes: abdominal discomfort, and epigastric discomfort. 6faeces soft includes: faeces soft and abnormal faeces. 7gastrointestinal motility disorder includes: gastrointestinal motility disorder, and frequent bowel movements. 8rash includes: rash, rash macular, rash erythematous, rash generalised, rash maculo-papular, rash papular, and urticarial. 9alanine aminotransferase increased includes: alanine aminotransferase increased and hepatocellular injury. Description of selected adverse reactions Immune reactivation syndrome In HIV‑infected patients with severe immune deficiency at the time of initiation of combination antiretroviral therapy (CART), an inflammatory reaction to asymptomatic or residual opportunistic infections may arise. Autoimmune disorders (such as Graves’ disease and autoimmune hepatitis) have also been reported; however, the reported time to onset is more variable and these events can occur many months after initiation of treatment (see section 4.4). Lactic acidosis Cases of lactic acidosis have been reported with tenofovir disoproxil alone or in combination with other antiretrovirals. Patients with predisposing factors such as patients with decompensated liver disease, or patients receiving concomitant medicinal products known to induce lactic acidosis are at increased risk of experiencing severe lactic acidosis during tenofovir disoproxil treatment, including fatal outcomes. Severe cutaneous adverse reactions (SCARs) Severe cutaneous adverse reactions (SCARs), such as toxic epidermal necrolysis (TEN), have been reported in association with doravirine-containing treatment regimens (see section 4.4). Paediatric population The safety of doravirine/lamivudine/tenofovir disoproxil was evaluated in 45 HIV-1 infected virologically suppressed or treatment-naïve paediatric patients 12 to less than 18 years of age through Week 48 in an open-label trial (IMPAACT 2014 (Protocol 027)). The safety profile in paediatric subjects was similar to that in adults. Reporting of suspected adverse reactions Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the national reporting system: In Belgium : Agence Fédérale des Médicaments et des Produits de Santé, www.afmps.be – Division Vigilance : Site internet: www.notifieruneffetindesirable.be, e-mail: adr@fagg-afmps.be, au Luxembourg : Centre Régional de Pharmacovigilance de Nancy ou Division de la pharmacie et des médicaments de la Direction de la santé. Site internet: www.guichet.lu/pharmacovigilance. 7. MARKETING AUTHORISATION HOLDER Merck Sharp & Dohme B.V., Waarderweg 39, 2031 BN Haarlem, The Netherlands. 8. MARKETING AUTHORISATION NUMBER(S) EU/1/18/1333/001, EU/1/18/1333/002. 9. DATE OF FIRST AUTHORISATION/RENEWAL OF THE AUTHORISATION Date of first authorisation: 22 November 2018; Date of latest renewal: 23 June 2023. 10. DATE OF REVISION OF THE TEXT 10/2025. Detailed information on this medicinal product is available on the website of the European Medicines Agency https://www.ema.europa.eu. DELIVERY: on medical prescription.
1. NAME OF THE MEDICINAL PRODUCT Pifeltro 100 mg film-coated tablets. 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Each film-coated tablet contains 100 mg of doravirine. Excipient with known effect: Each film-coated tablet contains 222 mg lactose (as monohydrate). For the full list of excipients, see section 6.1. 3. PHARMACEUTICAL FORM Film-coated tablet (tablet). White, oval-shaped, tablet of dimensions 19.00 mm x 9.50 mm, debossed with the corporate logo and 700 on one side and plain on the other side. 4. CLINICAL PARTICULARS 4.1 Therapeutic indications Pifeltro is indicated, in combination with other antiretroviral medicinal products, for the treatment of adults, and adolescents aged 12 years and older weighing at least 35 kg infected with human immunodeficiency virus type 1 (HIV‑1) without past or present evidence of resistance to the non-nucleoside reverse transcriptase inhibitors (NNRTI) class (see sections 4.4 and 5.1). 4.2 Posology and method of administration Therapy should be initiated by a physician experienced in the management of HIV infection. Posology The recommended dose is one 100 mg tablet taken orally once daily with or without food. Dose adjustment If Pifeltro is co-administered with rifabutin, one 100 mg tablet of Pifeltro should be taken twice daily (approximately 12 hours apart) (see section 4.5). Co-administration of doravirine with other moderate CYP3A inducers has not been evaluated, but decreased doravirine concentrations are expected. If co-administration with other moderate CYP3A inducers (e.g., dabrafenib, lesinurad, bosentan, thioridazine, nafcillin, modafinil, telotristat ethyl) cannot be avoided, one 100 mg tablet of Pifeltro should be taken twice daily (approximately 12 hours apart). Missed dose If the patient misses a dose of Pifeltro within 12 hours of the time it is usually taken, the patient should take as soon as possible and resume the normal dosing schedule. If a patient misses a dose by more than 12 hours, the patient should not take the missed dose and instead take the next dose at the regularly scheduled time. The patient should not take 2 doses at one time. Special populations Elderly No dose adjustment of doravirine is required in elderly patients (see section 5.2). Renal impairment No dose adjustment of doravirine is required in patients with mild, moderate, or severe renal impairment. Doravirine has not been studied in patients with end-stage renal disease and has not been studied in dialysis patients (see section 5.2). Hepatic impairment No dose adjustment of doravirine is required in patients with mild (Child-Pugh Class A) or moderate (Child-Pugh Class B) hepatic impairment. Doravirine has not been studied in patients with severe hepatic impairment (Child-Pugh Class C). It is not known whether the exposure to doravirine will increase in patients with severe hepatic impairment. Therefore, caution is advised when doravirine is administered to patients with severe hepatic impairment (see section 5.2). Paediatric population Safety and efficacy of Pifeltro in children aged less than 12 years or weighing less than 35 kg have not been established. No data are available. Method of administration Pifeltro must be taken orally, once daily with or without food and swallowed whole (see section 5.2). 4.3 Contraindications Hypersensitivity to the active substance or to any of the excipients listed in section 6.1. Co-administration with medicinal products that are strong cytochrome P450 CYP3A enzyme inducers is contraindicated as significant decreases in doravirine plasma concentrations are expected to occur, which may decrease the effectiveness of Pifeltro (see sections 4.4 and 4.5). These medicinal products include, but are not limited, to the following: carbamazepine, oxcarbazepine, phenobarbital, phenytoin; rifampicin, rifapentine; St. John’s wort (Hypericum perforatum); mitotane; enzalutamide; lumacaftor. 4.8 Undesirable effects Summary of the safety In phase 3 clinical trials with doravirine plus 2 nucleoside reverse transcriptase inhibitors (NRTIs), the most frequently reported adverse reactions were nausea (4 %) and headache (3 %). Tabulated summary of adverse reactions The adverse reactions with doravirine plus 2 NRTIs from Phase 3 clinical trials (DRIVE FORWARD, DRIVE SHIFT and DRIVE AHEAD) and postmarketing experience are listed below by body system organ class and frequency. Within each frequency grouping, undesirable effects are presented in order of decreasing seriousness. Frequencies are defined as very common (≥ 1/10), common (≥ 1/100 to < 1/10), uncommon (≥ 1/1 000 to < 1/100), rare (≥ 1/10 000 to < 1/1 000), or not known (cannot be estimated from the available data). Table 2: Tabulated summary of adverse reactions associated with doravirine used in combination with other antiretrovirals Frequency/ Adverse reactions: Infections and infestations: Rare: rash pustular. Metabolism and nutrition disorders: Uncommon: hypophosphataemia; Rare: hypomagnesaemia. Psychiatric disorders: Common: abnormal dreams, insomnia1; Uncommon: nightmare, depression2, anxiety3, irritability, confusional state, suicidal ideation; Rare: aggression, hallucination, adjustment disorder, mood altered, somnambulism. Nervous system disorders: Common: headache, dizziness, somnolence; Uncommon: disturbance in attention, memory impairment, paraesthesia, hypertonia, poor quality sleep. Vascular disorders: Uncommon: hypertension. Respiratory, thoracic and mediastinal disorders: Rare: dyspnoea, tonsillar hypertrophy. Gastrointestinal disorders: Common: nausea, diarrhoea, flatulence, abdominal pain4, vomiting; Uncommon: constipation, abdominal discomfort5, abdominal distension, dyspepsia, faeces soft6, gastrointestinal motility disorder7; Rare: rectal tenesmus. Hepatobiliary disorders: Not known: hepatitis. Skin and subcutaneous tissue disorders: Common: rash8; Uncommon: pruritus; Rare: dermatitis allergic, rosacea; Not known: toxic epidermal necrolysis. Musculoskeletal and connective tissue disorders: Uncommon: myalgia, arthralgia; Rare: musculoskeletal pain. Renal and urinary disorders: Rare: acute kidney injury, renal disorder, calculus urinary, nephrolithiasis. General disorders and administration site conditions: Common: fatigue; Uncommon: asthenia, malaise; Rare: chest pain, chills, pain, thirst. Investigations: Common: alanine aminotransferase increased9; Uncommon: lipase increased, aspartate aminotransferase increased, amylase increased, haemoglobin decreased; Rare: blood creatine phosphokinase increased. 1insomnia includes: insomnia, initial insomnia and sleep disorder. 2depression includes: depression, depressed mood, major depression, and persistent depressive disorder. 3anxiety includes: anxiety and generalised anxiety disorder. 4abdominal pain includes: abdominal pain, and abdominal pain upper. 5abdominal discomfort includes: abdominal discomfort, and epigastric discomfort. 6faeces soft includes: faeces soft and abnormal faeces. 7gastrointestinal motility disorder includes: gastrointestinal motility disorder, and frequent bowel movements. 8rash includes: rash, rash macular, rash erythematous, rash generalised, rash maculo-papular, rash papular, and urticarial. 9alanine aminotransferase increased includes: alanine aminotransferase increased and hepatocellular injury. Description of selected adverse reactions Immune reactivation syndrome In HIV‑infected patients with severe immune deficiency at the time of initiation of combination antiretroviral therapy (CART), an inflammatory reaction to asymptomatic or residual opportunistic infections may arise. Autoimmune disorders (such as Graves’ disease and autoimmune hepatitis) have also been reported; however, the reported time to onset is more variable and these events can occur many months after initiation of treatment (see section 4.4). Severe cutaneous adverse reactions (SCARs) Severe cutaneous adverse reactions (SCARs), such as toxic epidermal necrolysis (TEN), have been reported in association with doravirine-containing treatment regimens (see section 4.4). Paediatric population The safety of doravirine as a component of doravirine/lamivudine/tenofovir disoproxil was evaluated in 45 HIV-1 infected virologically suppressed or treatment-naïve paediatric patients 12 to less than 18 years of age through Week 48 in an open-label trial (IMPAACT 2014 (Protocol 027)). The safety profile in paediatric subjects was similar to that in adults. Reporting of suspected adverse reactions Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the national reporting system: in Belgium: Agence Fédérale des Médicaments et des Produits de Santé, www.afmps.be – Division Vigilance : Site internet: www.notifieruneffetindesirable.be, e-mail: adr@fagg-afmps.be, in Luxembourg : Centre Régional de Pharmacovigilance de Nancy ou Division de la pharmacie et des médicaments de la Direction de la santé. Site internet: www.guichet.lu/pharmacovigilance 7. MARKETING AUTHORISATION HOLDER Merck Sharp & Dohme B.V., Waarderweg 39, 2031 BN Haarlem, The Netherlands. 8. MARKETING AUTHORISATION NUMBER(S) EU/1/18/1332/001; EU/1/18/1332/002. 9. DATE OF FIRST AUTHORISATION/RENEWAL OF THE AUTHORISATION Date of first authorisation: 22 November 2018; Date of latest renewal: 07 July 2023 10. DATE OF REVISION OF THE TEXT 10/2025. Detailed information on this medicinal product is available on the website of the European Medicines Agency https://www.ema.europa.eu. DELIVERY: only on prescription.